Audience: biotech C-suites, program leaders, clinical pharmacology & modeling teams.
Why QSP matters now
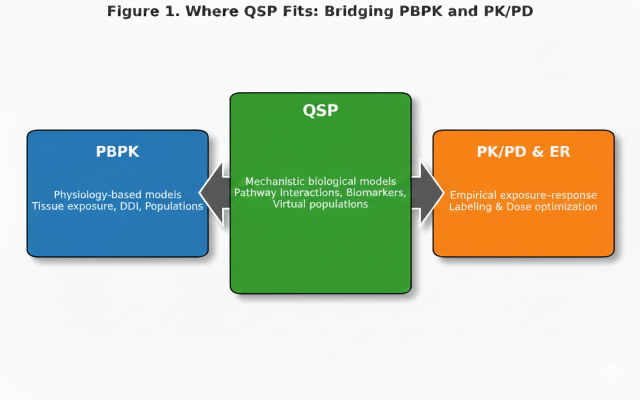
Sponsors increasingly face decisions where empirical models alone (PopPK, exposure–response) are not enough—novel mechanisms, combinations, complex biology, and heterogeneous populations. Quantitative Systems Pharmacology (QSP) integrates disease/biology knowledge with pharmacology to generate testable, decision-grade predictions across the translational and clinical continuum (e.g., dose/range selection, biomarker strategy, responder enrichment, virtual patient simulations) [1–3,6–7].
Regulators encourage model-informed drug development (MIDD). The FDA’s MIDD Pilot Program recognizes QSP as a tool to improve dose optimization and trial design; the EMA offers early engagement via ITF/Qualification Advice [1–3]. QSP does not replace PBPK or PopPK; it connects them, enabling mechanistic inference that complements empirical analyses.
QSP within the model-informed continuum
Positioning QSP alongside PBPK and PopPK clarifies roles and expectations [1–2,6–7].
| Approach | Focus | Typical outputs | Strengths | Limitations |
|---|---|---|---|---|
| PBPK | Physiologic distribution & ADME | Organ exposures, DDIs, special populations | Mechanistic PK; established regulatory expectations | Limited direct PD insight |
| PopPK / ER | Statistical exposure–response | Covariate effects, variability, dose justification | Empirical precision; label-relevant | Limited mechanistic extrapolation |
| QSP | Mechanistic biology–pharmacology integration | Biomarker predictions, virtual trials, mechanistic dose response | Causal inference; translational bridge | Data & resource intensive; scope management needed |
When to employ QSP (fit for purpose)
QSP is a powerful but specialized tool, not a universal solution for every pharmacology or translational question. Its greatest strength lies in providing mechanistic clarity where empirical data cannot reach, but it requires significant investment in data generation, expertise, and time.
When it makes sense
QSP adds clear value when:
- Mechanistic uncertainty dominates. This includes novel modalities such as bispecific antibodies, ADCs, RNA and gene therapies, or new combinations where biological feedback and cross talk are not well understood.
- Data are sparse or fragmentary. QSP can integrate in vitro, preclinical, and early clinical information to project human responses or to rationalize divergent findings across studies.
- High stakes decisions loom. First in human dose, proof of concept design, or dose justification for pivotal trials all benefit from transparent mechanistic reasoning.
- Multiple hypotheses compete. QSP enables scenario testing and prioritization before committing to resource intensive studies.
When it may not be the right tool
QSP is not a cure all, and sponsors should avoid using it by default. It may not be the right choice if:
- The biology is well characterized and rich clinical data are available. In such cases a PopPK or exposure response model can often provide the needed justification faster and at lower cost.
- Timelines are tight and only minimal in vitro characterization exists, limiting calibration and insight.
- The question is mainly empirical, for example comparing formulations or evaluating small dose adjustments, where empirical PK/PD approaches are more efficient.
Balancing scientific and practical considerations
Implementing QSP requires upfront investment, often several months of dedicated effort and a multidisciplinary team. Key practical factors include:
- Data prerequisites: high quality in vitro kinetic data, target expression, turnover, and biomarker information. Without these, calibration becomes speculative.
- Cross functional collaboration: modelers, pharmacologists, and biologists must iterate together. Outsourcing without internal oversight risks models misaligned with program reality.
- Cost benefit assessment: a fit for purpose model can be built within modest budgets (hundreds of thousands of dollars) if its scope is well constrained and aligned to a specific decision.
- Regulatory credibility: both FDA and EMA expect transparent model reporting. Black box or overly theoretical models rarely influence decisions.
Advantages for smaller biotechs
For small and mid size companies, QSP can be a strategic equalizer by providing the quantitative depth that larger organizations achieve through multiple exploratory studies. When executed carefully it can:
- Strengthen scientific narratives for investors and partners by demonstrating mechanistic rationale.
- Reduce the need for duplicative preclinical work by integrating public or partner data.
- Provide transparent justification for dose and biomarker strategy in early regulatory interactions.
Cautions
Realism is essential. QSP requires sustained access to data and iterative refinement; it cannot fill in missing experimental evidence. Overextending model complexity beyond available data can create the illusion of precision without predictive value.
Ultimately, the key question is not Can we build a QSP model? but Will a QSP model improve the decision we must make? When used for the right purpose, and with realistic expectations, QSP remains one of the most effective ways to combine biology, pharmacology, and quantitative reasoning in modern development.

Selected real-world examples
- Immunology: QSP of epithelial cytokine network (e.g., TSLP axis) to compare pathway blockade strategies; informed Phase 2 dose and biomarker selection [6].
- Oncology (ADCs): hybrid PBPK–QSP models linking tumor exposure and payload kinetics to response; narrowed FIH dose ranges [6–7].
- Rare disease / gene therapy: QSP linked transduction/expression to substrate dynamics; supported dose selection and spacing under ethical constraints [6–7].
Data requirements & credibility
High-impact, regulatory-ready QSP requires disciplined scope, calibration, validation, and uncertainty analysis. FDA/EMA emphasize transparency, traceability, and reproducibility—principles aligned with PBPK guidance and model credibility frameworks [1–3].
Table 1. QSP data & resource requirements
| Component | Typical sources | Key considerations |
|---|---|---|
| Biological network map | Literature, pathway databases, omics | Scope control; explicit assumptions; versioned diagrams |
| Parameterization | In-vitro kinetics, animal PK/PD, clinical PK | Scaling rules; identifiability; biological plausibility |
| Calibration | Time-course biomarkers, PD endpoints | Optimization/Bayesian inference; cross-validation; avoid overfit |
| Validation | Independent datasets or prospective checks | Quantitative checks (e.g., VPCs); pre-specified acceptance limits |
| Sensitivity & uncertainty | Local/global methods; Monte-Carlo | Identify drivers; scenario robustness; communicate uncertainty |
| Integration with PBPK/PopPK | Tissue exposures, systemic PK models | Compartment alignment; units; data lineage |
| Documentation & traceability | Version-controlled code, metadata, logs | Reproducibility; audit trail; submission-ready packaging |
Effort, timing, and budget (what sponsors should plan)
Effort depends on question complexity and data maturity; below are typical ranges for small/mid-size biotech programs (externalized or hybrid staffing). These align with best-practice reports and regulatory expectations for model credibility [1–3].
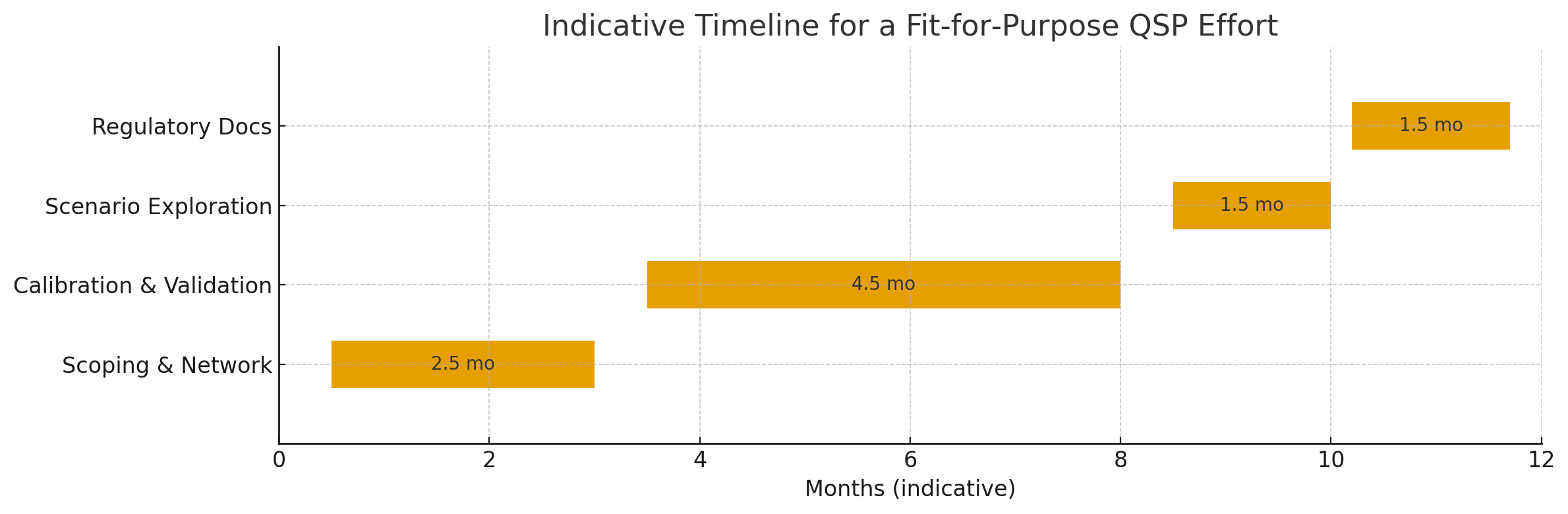
Table 2. Indicative cost & timeline ranges (biotech context)
| Phase | Typical duration | Approx. cost (USD) | Notes |
|---|---|---|---|
| Scoping & network definition | 1–2 months | $100k–$200k | Target complexity & data maturity dependent |
| Model development & calibration | 3–5 months | $150k–$400k | Biology–PK alignment; parameter priors and inference strategy |
| Validation & scenario testing | 2–3 months | $50k–$150k | Independent datasets; global sensitivity; virtual populations |
| Reporting & regulatory documentation | ~1 month | $50k–$100k | Module 2.7.2 summary; full 5.3.3.1 report; briefing materials |
Regulatory guidance & submission considerations
Agencies support MIDD and regularly discuss QSP in scientific advice. While there is no single “QSP format,” expectations are documented through MIDD pilots, PBPK guidance, and EMA reflections on MIDD [1–3]. QSP material typically appears in CTD Module 2.7.2 (summary) with full reports in Module 5.3.3.1, and integration into Module 2.5 at NDA/BLA [1–2].
Table 3. Regulatory guidance summary (concise): FDA | EMA | PMDA
| Aspect | FDA | EMA | PMDA |
|---|---|---|---|
| Primary framework | MIDD Pilot Program | ITF / Qualification Advice | Innovation / Sakigake pathways |
| Model credibility | Transparency, PBPK & V&V-40 principles | Alignment with EMA Reflection Paper | Consistency with clinical relevance |
| Placement in CTD | 2.7.2 summary; 5.3.3.1 full report; 2.5 overview | 2.7.2 or annex to ITF/Qualification | Follows ICH CTD structure |
| Engagement timing | Pre-IND or EoP1 Type C | Pre-IND ITF; early scientific advice | Case-by-case before clinical |
| Key expectations | Validation, uncertainty analysis, traceability | Clear context of use; regulatory transparency | Integration with local clinical data |
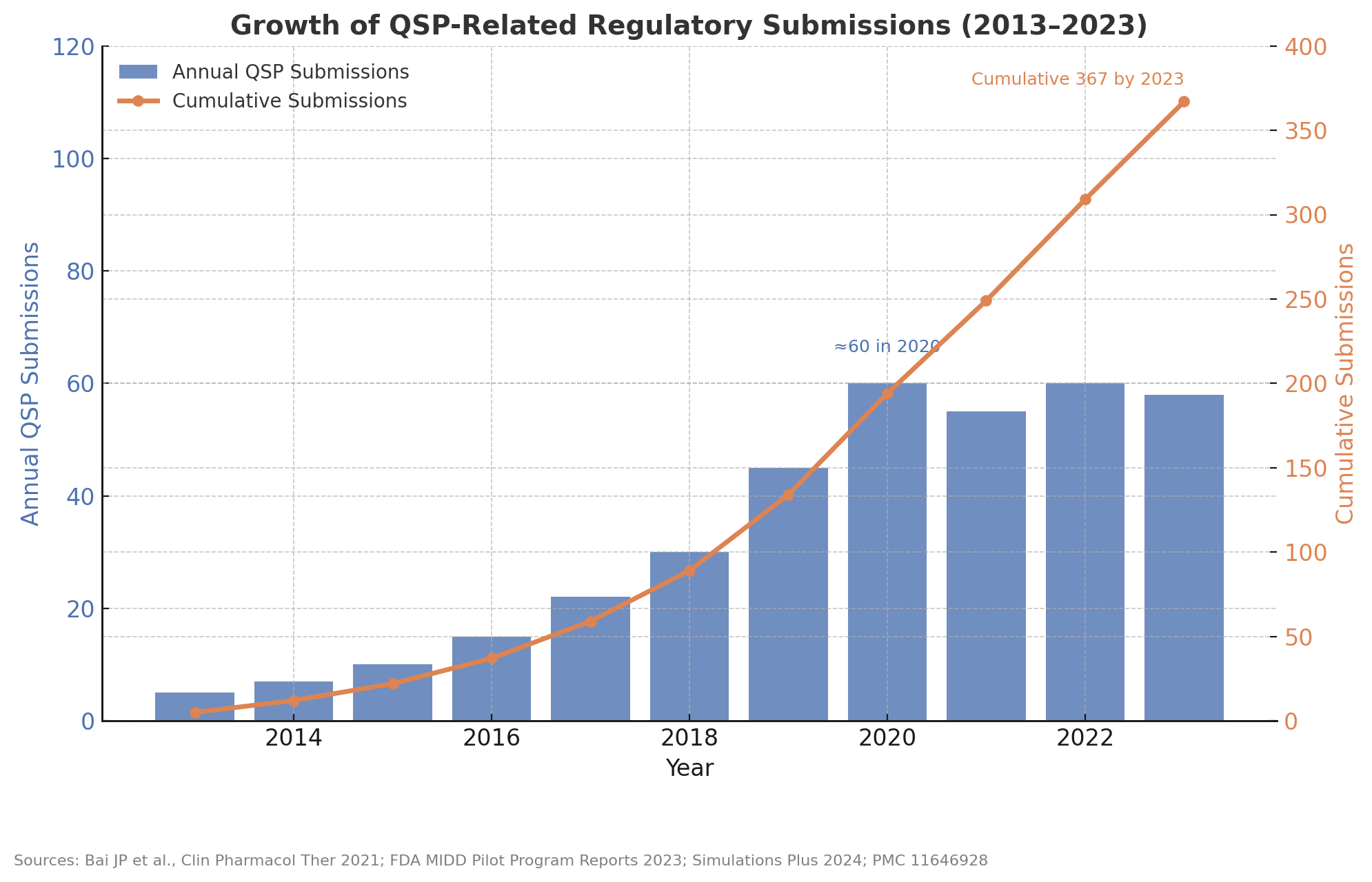
Adoption trends
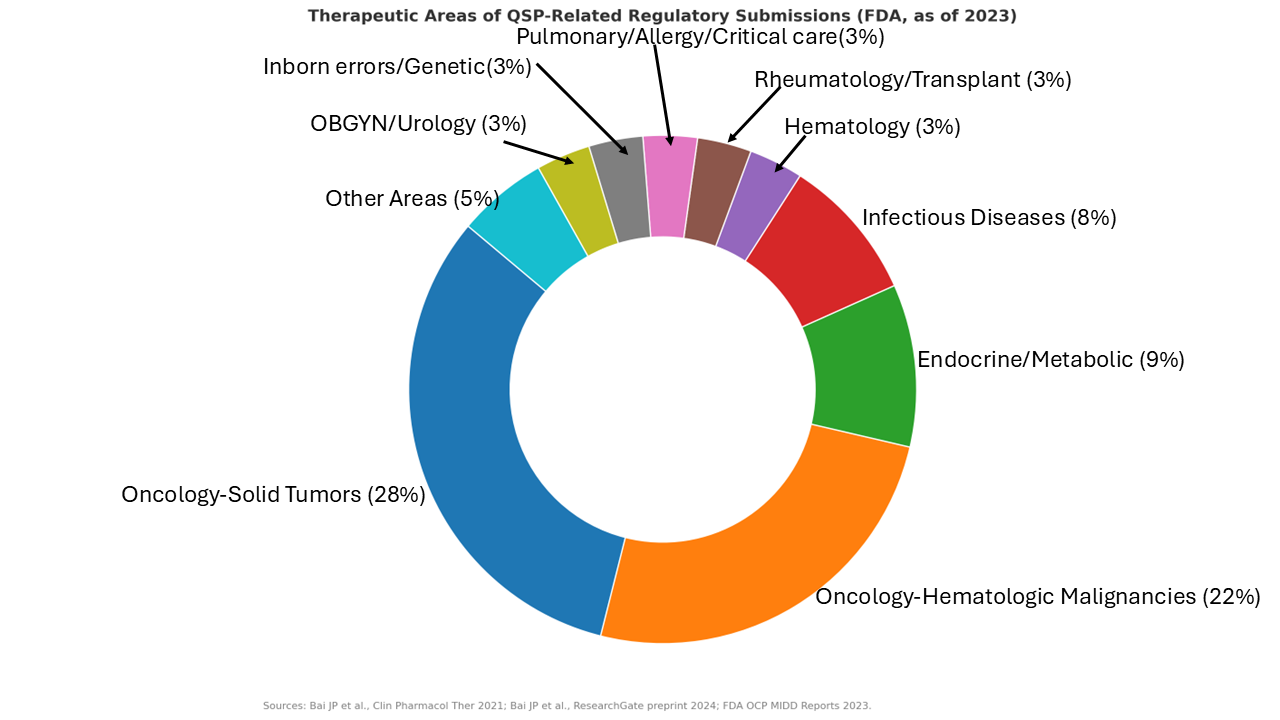
Public updates indicate a steady increase in QSP-containing submissions to FDA since ~2013, reaching several hundred cumulatively by 2023. Oncology dominates by share, followed by endocrine/metabolic and infectious disease, with smaller but growing contributions across other areas [4–5].
Where QSP is used most
Oncology accounts for the largest share of QSP submissions, with meaningful activity in endocrine/metabolic and infectious diseases. Other areas (e.g., pulmonary/allergy, rheumatology, non-malignant hematology, inborn errors) contribute smaller but growing proportions [4–5].
How ClinPharm Dev Solutions can help
- Program-level QSP strategy: fit-for-purpose scoping; integration with PBPK/PopPK/ER and clinical pharmacology.
- Build or oversee QSP work: partner/vendor oversight, quality gates, reproducibility and documentation.
- Regulatory-ready packages: author Module 2.7.2 and 5.3.3.1 sections; MIDD proposals; EMA ITF/Qualification material [1–3].
- Decision impact: FIH dose strategies, biomarker/endpoint recommendations, and Phase 2/3 trial design insights.
References
- FDA Model-Informed Drug Development (MIDD) Program. Public descriptions and updates outlining how modeling (including QSP) is considered in regulatory interactions.
- FDA Guidance for Industry: Physiologically Based Pharmacokinetic (PBPK) Analyses—Format and Content. 2023.
- EMA Reflection Paper on the use of modelling and simulation in the context of clinical development and licensing of medicines (Model-Informed Drug Development). 2022.
- Bai JP, et al. Landscape of regulatory QSP submissions to the U.S. FDA. Clin Pharmacol Ther. 2021.
- Bai JP, et al. Update on the landscape of regulatory QSP submissions (through 2023). CPT: Pharmacometrics & Systems Pharmacology. 2024.
- Musante CJ, et al. Quantitative Systems Pharmacology: a framework for integrating biology and pharmacology to support decision making. CPT: Pharmacometrics & Systems Pharmacology. 2016.
- NIH QSP White Paper / Community Reports. Foundational perspectives on QSP goals, model credibility, and integration into R&D decision-making.
Abbreviations
- QSP: Quantitative Systems Pharmacology
- PBPK: Physiologically Based Pharmacokinetics
- PopPK: Population Pharmacokinetics
- ER: Exposure–Response
- FIH: First-in-Human
- MIDD: Model-Informed Drug Development
- ITF: Innovation Task Force (EMA)
- CHMP: Committee for Medicinal Products for Human Use (EMA)
- CTD: Common Technical Document
- TPP: Target Product Profile