While small molecules represent the foundational pillar of systemic pharmacotherapy, the regulatory landscape of 2026 demands a departure from empirical dose-finding. This report details the comprehensive requirements of a modern small molecule Clinical Pharmacology Plan (CPP), spanning biopharmaceutics, classical ADME, metabolic liabilities, and the Model-Informed Drug Development (MIDD) engine.
| Article Sequence | Thematic Focus | Status |
|---|---|---|
| Article 1 | Overview of Modalities and the Clinical Pharmacology Plan | Published |
| Article 2 | Small Molecule PK and Bioavailability | Current Report |
| Article 3 | Large Molecule Biologics and Subcutaneous Delivery | Upcoming |
Introduction: The Evolution of Small Molecule Development
Small molecule therapeutics remain a cornerstone of modern medicine; however, their development has moved past empirical trial-and-error toward a highly mechanistic discipline. The success of an investigational small molecule is now contingent upon a robust Clinical Pharmacology Plan (CPP) that integrates physicochemical properties, metabolic pathways, and advanced mathematical modeling to validate the “Three Pillars of Survival.”
Section 1: Biopharmaceutics and Formulation Strategy
The foundation of the CPP is ensuring the physical properties of the active pharmaceutical ingredient do not artificially limit its systemic exposure. The Biopharmaceutics Classification System (BCS) serves as the primary guide for formulation strategy.
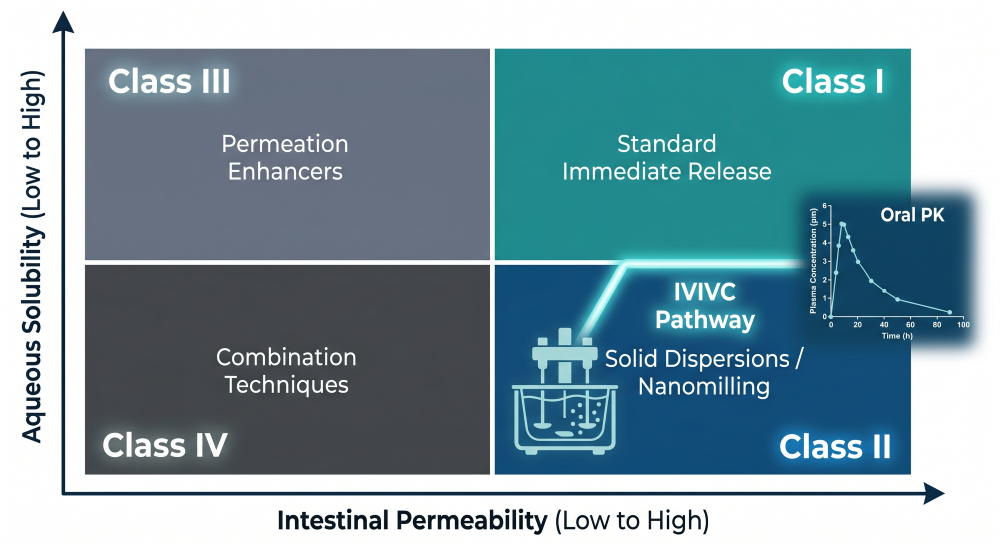
Figure 1: The BCS Strategic Matrix — Formulation Pathways and IVIVC Objectives
For Class II and Class III molecules, enhancement techniques such as nanomilling or amorphous solid dispersions are deployed. A critical objective is establishing an In Vitro-In Vivo Correlation (IVIVC), allowing developers to secure regulatory biowaivers for future manufacturing changes.
Section 2: Pharmacokinetic Characterization and Mechanistic Absorption
The empirical foundation relies on a rigorous assessment of Absorption, Distribution, Metabolism, and Excretion (ADME). This begins with Single and Multiple Ascending Dose (SAD/MAD) studies to characterize PK linearity and dose proportionality. Concurrently, a mass balance study defines primary excretion routes and identifies major metabolites. Modern CPPs utilize Advanced Compartmental Absorption and Transit (ACAT) models to simulate in vivo dissolution and predict the magnitude of food effects prior to pivotal trials.
Section 3: Extrinsic Factors and Metabolic Liabilities (DDI)
Small molecules are uniquely susceptible to metabolic interference. The CPP identifies the drug as a victim or perpetrator of Cytochrome P450 (CYP) and transporter-mediated interactions.
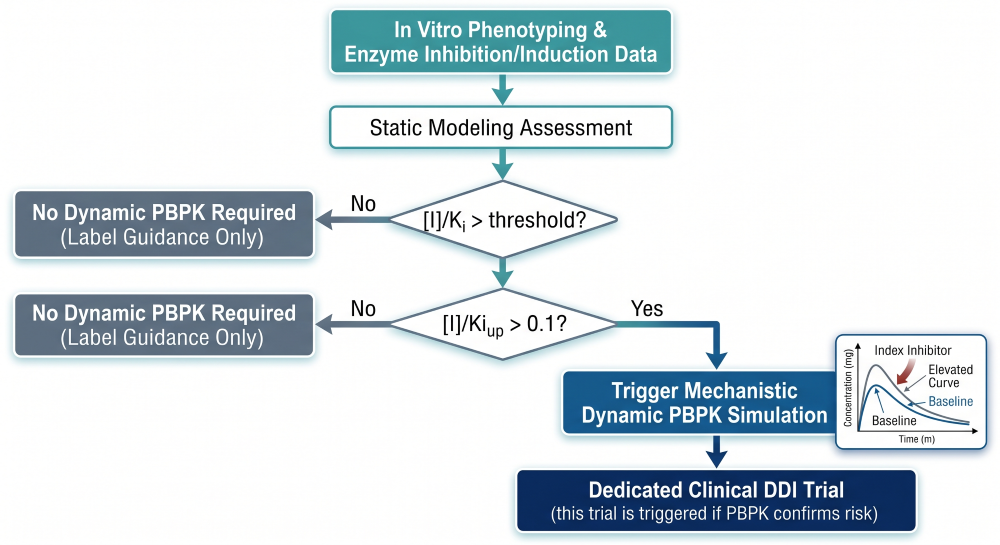
Figure 2: Risk Assessment Framework — Transitioning from In Vitro to Dynamic PBPK DDI Modeling
Static prediction models lead to dynamic Physiologically Based Pharmacokinetic (PBPK) simulations. If thresholds are crossed, targeted clinical trials with index inhibitors or cocktail studies are executed to quantify the interaction magnitude and inform product labeling.
Section 4: Intrinsic Factors and The Hepatic-Renal Paradox
The CPP must address physiological variations, including renal and hepatic impairment. For BDDCS Class 2 lipophilic molecules, the 2026 framework mandates assessing the “hepatic-renal paradox.”
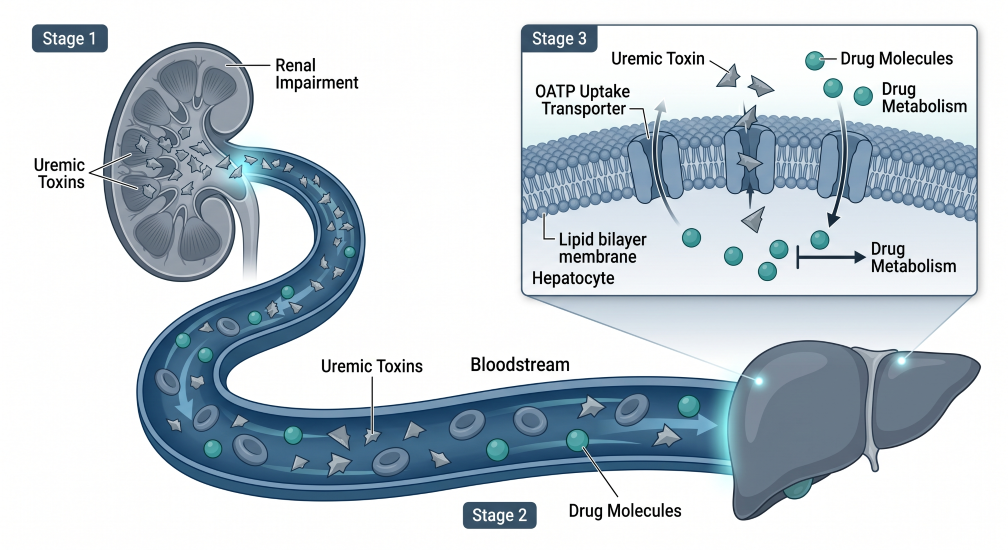
Figure 3: Uremic Toxin Modulation — Indirect Inhibition of Hepatic Transporters in Renal Impairment
Renal failure causes uremic toxins to accumulate in the bloodstream, which travel to the liver and block uptake transporters (OATP). This mechanism indirectly reduces hepatic metabolic capacity, requiring specific dose adjustments for renal patients even when the drug is not primarily renally cleared.
Section 5: The MIDD Engine (Modeling and Simulation)
Modeling and Simulation (M&S) is the core analytical engine. It synthesizes ADME data with population-level variability to justify the final dosing regimen.
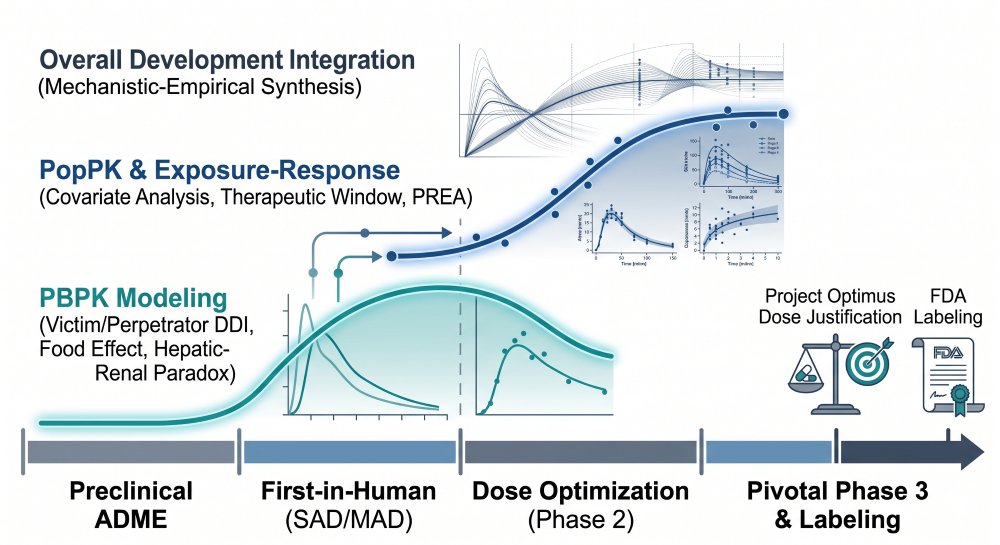
Figure 4: The M&S Continuum — Integration of PBPK, PopPK, and E-R Modeling Across the Lifecycle
PBPK predicts unstudied scenarios, while Population Pharmacokinetics (PopPK) identifies critical covariates. Exposure-Response (E-R) modeling establishes the therapeutic window, linking systemic levels directly to efficacy and safety outcomes. Pediatric scaling utilizes these models to fulfill PREA requirements through allometric bridging.
Section 6: Pharmacodynamics and Cardiac Safety
Modern cardiac safety assessments utilize Concentration-QTc (cQTc) modeling. By applying intensive ECG monitoring and PK sampling during Phase 1, developers can mathematically rule out QTc prolongation, frequently securing a regulatory waiver for dedicated Thorough QT (TQT) studies.
Summary of Small Molecule CPP Components
| CPP Component | Regulatory Objective | M&S Tool |
|---|---|---|
| Biopharmaceutics | Secure biowaivers; optimize formulation. | IVIVC Modeling |
| Absorption | Define food effect and labeling. | ACAT / PBPK |
| DDI Profiling | Mitigate polypharmacy risks. | Static / Dynamic PBPK |
| Special Pops | Dosing for organ impairment/pediatrics. | PopPK / Allometry |
| Cardiac Safety | Rule out QTc liabilities. | cQTc Modeling |
Abbreviations
ACAT: Advanced Compartmental Absorption and Transit
BCS: Biopharmaceutics Classification System
CPP: Clinical Pharmacology Plan
cQTc: Concentration-QTc
CYP: Cytochrome P450
DDI: Drug-Drug Interaction
E-R: Exposure-Response
IVIVC: In Vitro-In Vivo Correlation
MIDD: Model-Informed Drug Development
PBPK: Physiologically Based Pharmacokinetic
PopPK: Population Pharmacokinetics
PREA: Pediatric Research Equity Act
Technical References
- FDA Guidance (2026). Pharmacokinetics in Patients with Impaired Renal Function.
- FDA Guidance (2025). Clinical Drug Interaction Studies — Transporter-Mediated Interactions.
- ICH E14/S7B Implementation Guide (2024). Clinical Evaluation of QT/QTc Interval Prolongation.
- Amidon, G. L., et al. (1995). A Theoretical Basis for a Biopharmaceutic Drug Classification.
- Rowland, M., et al. (2011). Physiologically Based Pharmacokinetics in Drug Development.